
When we talk about “patient engagement” in research, it can sound like a slogan on a grant application rather than something that changes people’s lives.
Across Canada and many other countries, funding agencies now ask researchers to involve patients in their studies. In theory, this should make health research more relevant, equitable and easier to apply in real-world care. In practice, however, engagement is often limited to asking a patient to review a document, join an advisory committee in name only, or attend a single meeting where decisions have already been made.
Patients are invited into the room—but not into the work.
My colleagues and I wanted to do something different.
Why women’s voices are missing from cardiac rehabilitation
Cardiovascular disease is the leading cause of death among women worldwide. Cardiac rehabilitation (CR)—secondary prevention programs that combine exercise, education and psychosocial support—can reduce deaths and hospitalizations and help people return to their lives after a heart event.
Yet women are consistently less likely than men to be referred to CR, to enroll, or to stay long enough to benefit. Many tell us that the programs and educational materials do not really feel “for them”: They see mostly male examples and images, language that does not reflect their lives and responsibilities, and limited acknowledgment of their emotional experiences.
If women’s realities are absent from the way we teach and support them, it is not surprising that participation remains low.
From feedback to co-design
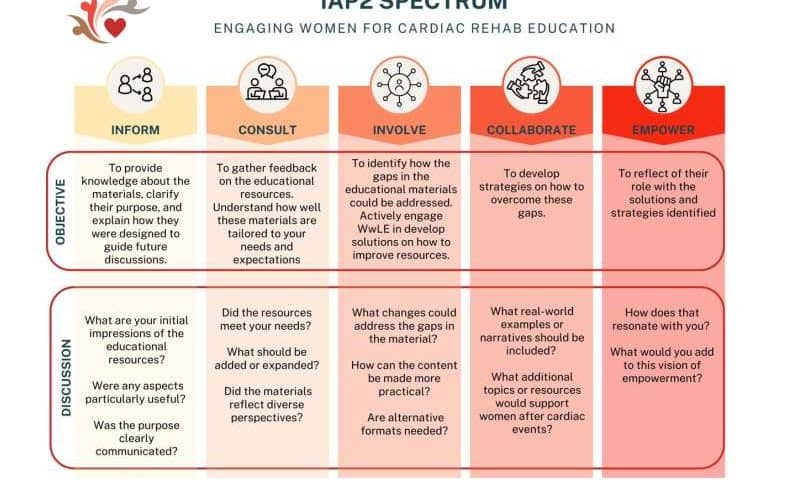
In our recent study published in Patient Education and Counseling, we invited 11 women with lived experience of cardiovascular disease—some who had attended CR, some who had not—to help refine the educational resources in the Cardiac College for Women, a web-based curriculum developed at University Health Network (Toronto, Canada).
Instead of a single consultation, we organized five online workshops over several months. We used established engagement frameworks to deliberately shift power over time. A woman with lived experience co-facilitated the workshops. Participants were compensated for their time, received summaries between sessions, and saw their suggestions incorporated in real time. We measured engagement using validated scales, but perhaps the most powerful evidence came from their comments: Many said they felt heard, respected and “part of something that will help other women like me.”
What patients changed—and why it matters
The women identified five priority areas for improvement:
- Accessibility. Navigation needed to be clearer, the language simpler, and the fonts larger. They asked for audio options and visual summaries for those who struggle with long blocks of text.
- Storytelling. Facts alone were not enough. Hearing how other women coped with fear, fatigue and caregiving responsibilities made information memorable and motivating.
- Representation. They wanted more diverse images and stories—different ages, ethnicities, body types, family structures and financial realities—so that more women could “see themselves” in the materials.
- Multiple formats. Some preferred short videos, others printable handouts, others audio they could listen to while walking. A single format could never serve everyone.
- Reaching more women. They proposed practical ways to share the materials: through cardiologists and family doctors, community organizations, pharmacies and social media.
These are not minor cosmetic tweaks. They reshape who the materials are for, how they are experienced and which women are most likely to benefit.
Tokenism vs. meaningful engagement
What made this process feel different from tokenistic engagement?
- Real influence. Participants saw their ideas adopted—sometimes word-for-word. They were not just “advising”; they were co-creating.
- Psychological safety. Ground rules were set together. People could disagree respectfully. Emotions were acknowledged, not brushed aside.
- Continuity. We met repeatedly, built relationships, and checked back after each session. Engagement was a process, not a one-time event.
- Recognition. Women were compensated, named as contributors, and invited to continue as partners in future work.
Meaningful engagement takes more time and planning than sending a survey link. But it also produces better science. The women highlighted issues we would not have identified on our own and suggested solutions that were practical and grounded in real life.
Beyond our project: A better way to do health research
Our study focused on women in cardiac rehabilitation, but the lessons are broader.
When patients are treated as partners rather than passive subjects, research questions become more relevant, interventions are easier to implement, and findings are more likely to reduce inequities rather than reinforce them. This is especially important for groups that have historically been excluded from research—women, racialized communities, people with lower incomes or disabilities.
For researchers, the challenge is to move from “checking the engagement box” to genuinely sharing power:
- Invite patients in early, when there is still room to shape the project.
- Be transparent about what they can influence—and follow through.
- Create structures (like repeated workshops, clear roles and fair compensation) that support ongoing, respectful collaboration.
Patients are more than participants. They are experts in their own lives and essential partners in designing health systems that truly work for everyone. Our experience with women living with heart disease shows that when we listen carefully—and are prepared to act on what we hear—research becomes not only more just, but more effective.